
A wound that will not heal is rarely a surface-level problem. Clinicians often respond to stalled wounds by changing dressings, increasing debridement, or escalating to advanced therapies. These are appropriate steps. But when a wound appears technically well managed and still fails to progress, the issue is often deeper.
Chronic wound healing factors are largely systemic. Perfusion, oxygenation, inflammation, metabolic control, and medication exposure determine whether tissue can actually respond to treatment.
This article breaks down why wounds stall, how systemic physiology drives outcomes, and what to evaluate before escalating care.
Why Some Wounds Do Not Heal Despite Proper Care
Surface-Level Treatment vs Underlying Physiology
Topical management addresses the wound environment. It does not correct the biologic conditions required for healing.
A perfectly selected dressing cannot compensate for poor arterial inflow.
An advanced graft cannot integrate into hypoxic tissue.
When systemic conditions are misaligned, local interventions plateau.
Signs a Wound Is Stalled or Plateaued
Recognizing stagnation early is critical. Common indicators include:
- Stable but non-progressing wound size
- Persistent inflammation without transition to proliferation
- Fragile epithelial edges that repeatedly break down
- Granulation tissue that forms but does not mature
These are not failures of care. They are signals of physiologic limitation.
When Dressing Changes and Debridement Are Not Enough
Escalation without reassessment creates activity without progress.
If a wound remains “busy but not better,” the clinical question shifts from what are we applying to what is preventing response.
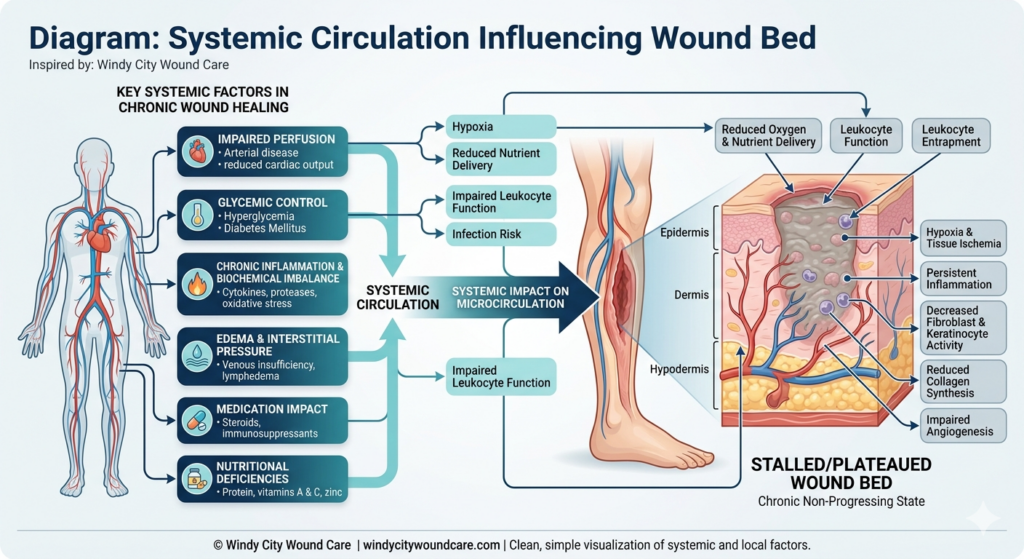
Key Systemic Factors in Chronic Wound Healing
Impaired Perfusion and Oxygen Delivery
Peripheral arterial disease restricts oxygen and nutrient delivery. Without adequate perfusion:
- Fibroblast activity declines
- Collagen deposition weakens
- Tissue regeneration slows or stops
Even minor perfusion deficits can significantly delay healing.
Glycemic Control and Leukocyte Function
Hyperglycemia disrupts immune function and increases infection risk. It impairs:
- Neutrophil activity
- Cytokine signaling
- Microvascular circulation
According to American Diabetes Association, uncontrolled glucose levels are a primary contributor to delayed wound healing.
Chronic Inflammation and Biochemical Imbalance
Chronic wounds often remain trapped in an inflammatory phase. Elevated proteases degrade growth factors and extracellular matrix components, preventing progression.
Research supported by National Institutes of Health highlights the role of persistent inflammation in stalled healing.
Edema and Interstitial Pressure
Fluid accumulation increases tissue pressure, reducing capillary flow. This leads to:
- Impaired oxygen diffusion
- Cellular dysfunction
- Increased risk of breakdown
Edema is frequently underestimated but clinically significant.
Medication Impact
Certain medications directly suppress healing mechanisms:
- Corticosteroids reduce collagen synthesis
- Immunosuppressants blunt inflammatory response
- Some antibiotics impact cellular proliferation
Medication review is a necessary step in non-healing wounds.
Nutritional Deficiencies
Protein, vitamin C, zinc, and micronutrients are essential for tissue repair.
Deficiencies impair:
- Fibroblast function
- Angiogenesis
- Collagen formation
Malnutrition is common and often overlooked.
How Systemic Physiology Directly Impacts the Wound Bed
Why Poor Perfusion Prevents Regeneration
Tissue cannot rebuild without oxygen and substrate delivery. Perfusion is the foundation of healing, not an adjunct.
The Role of Oxygenation in Cellular Repair
Oxygen drives:
- ATP production
- Collagen cross-linking
- Bacterial control
Low oxygen states shift wounds into chronicity.
Why Advanced Therapies Fail Without Optimization
Biologic grafts, NPWT, and advanced modalities rely on a responsive environment.
Without systemic alignment:
- Grafts fail to integrate
- Tissue remains unstable
- Outcomes plateau
Technology does not override physiology.
Clinical Indicators That Systemic Factors Are Being Missed
“Well-Managed” but Non-Progressing Wounds
Frequent interventions with minimal improvement signal underlying issues.
Recurrent Breakdown
Wounds that close and reopen indicate unstable tissue integrity.
Granulation Without Maturation
Healthy granulation must transition to epithelialization. When it does not, systemic barriers are likely present.
When to Refer for Advanced Wound Care Evaluation
Referral Criteria
Consider referral when:
- No measurable improvement in 2 to 4 weeks
- Recurrent or complex wounds
- Suspected vascular compromise
- Multimorbidity complicating care
Multidisciplinary Oversight
Advanced wound care integrates:
- Vascular assessment
- Metabolic optimization
- Local wound management
Organizations like Society for Vascular Surgery emphasize early vascular evaluation in non-healing wounds.
Benefits of Early Intervention
Early referral reduces:
- Hospital readmissions
- Infection risk
- Time to closure
Delays compound complexity.
A Broader Approach to Chronic Wound Management
Integrating Systemic and Local Care
Effective care aligns:
- Perfusion
- Metabolic control
- Inflammation management
- Local wound environment
Coordinating Across Providers
Collaboration with primary care, endocrinology, and vascular specialists improves outcomes.
Simplifying Before Escalating
More treatment is not always better.
Reducing interference and stabilizing conditions often produces better results than adding therapies.

