A family member changes a dressing and notices something unsettling. The skin opening doesn’t look especially large, but the wound seems deeper than it should. Drainage keeps returning. The area may have an odor, or the patient says the pain feels “deeper” than the surface suggests. That’s often the moment people start asking the right question: what is a tunneling wound, and how serious is it?
It’s a serious question because some wounds are far more extensive below the skin than they appear from above. In practice, these wounds need careful assessment, a structured treatment plan, and consistent follow-through at home. Surface care alone usually isn’t enough.
Defining the Unseen What Is a Tunneling Wound
A tunneling wound can look deceptively small at the skin surface while extending into deeper tissue underneath. In home care, that mismatch is what creates trouble. Families often judge the wound by the opening they can see, but treatment decisions depend on the hidden tract, the tissue it passes through, and whether drainage or infection is collecting below the surface.
A tunneling wound is a wound with a narrow channel or tract that extends from the visible wound bed into deeper tissue. That tract may travel straight, curve, or branch. The surface opening may appear modest even when the internal wound is more extensive.
How tunneling differs from undermining
Clinicians separate tunneling from undermining because each pattern changes the care plan. Tunneling is a narrow, more defined passage into deeper tissue. Undermining is tissue loss beneath the wound edge that creates a broader shelf or pocket rather than a single tract.
The distinction is clinically important because packing technique, dressing selection, monitoring, and the risk of trapped drainage are different in each case. If you want a broader primer on wound categories, this guide to the 6 types of wounds helps place tunneling wounds in context.
Practical rule: If the wound opening looks small but the drainage persists, the odor worsens, the pain feels deeper, or healing stalls, treat the wound as potentially more complex than it appears until a clinician maps it properly.
Why these wounds demand respect
A tunneling wound has concealed extension. That changes day-to-day care at home. Surface cleaning alone will not address dead space under the skin, and a dressing that looks adequate from the outside may miss the area that is driving drainage, inflammation, or delayed healing.
This is also where families and primary care teams can miss early warning signs. A wound may seem stable because the opening has not enlarged, while the tract is still present or getting worse. In practice, these wounds call for careful assessment, deliberate treatment, pressure relief when indicated, and close follow-through between clinic visits and dressing changes at home.
For patients and caregivers, the key point is simple. A tunneling wound is a wound with hidden depth, and hidden depth changes how the wound is cleaned, packed, monitored, and escalated when red flags appear.
How Clinicians Assess Tunneling Wounds
The first good wound visit often feels more methodical than people expect. A clinician doesn’t just look at the surface and choose a dressing. The actual work starts with defining the wound’s shape, depth, direction, and tissue quality.
What happens during the exam
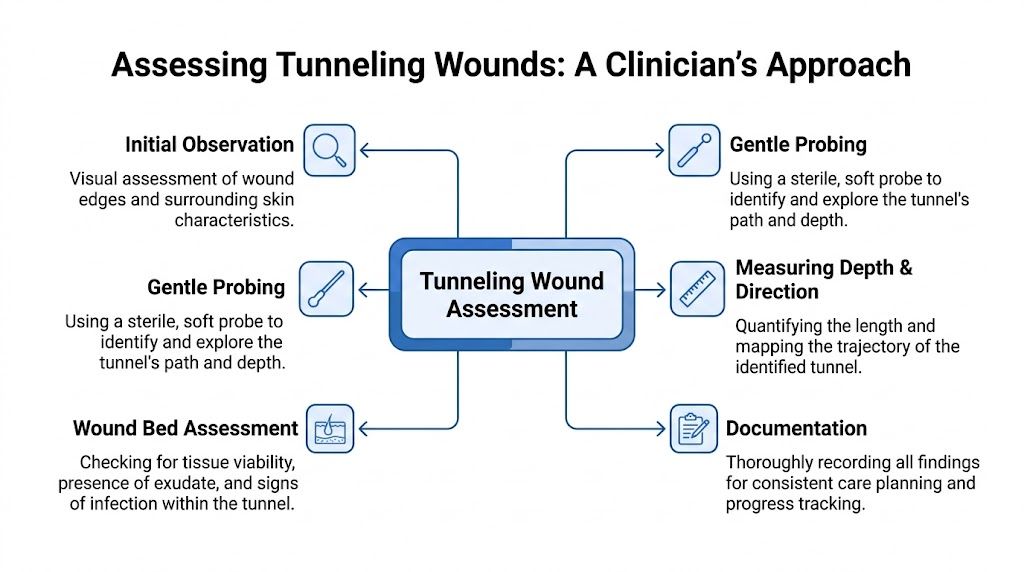
Assessment begins with direct observation. The clinician looks at the wound bed, the edges, the surrounding skin, the drainage pattern, and whether the area suggests pressure, moisture injury, friction, or infection. The visible opening is only the starting point.
Then comes gentle probing. A trained wound clinician typically uses a soft, sterile probe or catheter to explore the tract. The purpose is to identify:
- How deep it goes
- Which direction it travels
- Whether there are branches or dead ends
- Whether the tissue feels firm, friable, boggy, or irregular
This isn’t random poking. It’s a controlled assessment designed to map the wound safely. A practical overview of wound assessment tools helps explain why standardized measurement matters so much in chronic wound care.
Why documentation is so specific
Once the tunnel is identified, the clinician documents it in a repeatable way. Many teams use the clock method. A tunnel might be described by position and depth, such as a tract extending at a certain o’clock location from the wound center. That standardization allows nurses, physicians, podiatrists, and home health teams to talk about the same structure clearly across visits.
A tunneling wound can’t be managed well if it hasn’t been mapped well.
The assessment also looks for tissue and fluid behavior inside the tract. Is there thick drainage suggesting a retained pocket? Is there slough or necrotic debris that will block healing? Is the surrounding tissue macerated because the dressing isn’t handling moisture well? Those findings shape the treatment plan immediately.
What clinicians are trying to avoid
A missed tunnel leads to missed dead space. Dead space gives fluid and bacteria room to collect. That’s one reason these wounds stall.
During a proper assessment, the clinician is also deciding whether bedside management is appropriate or whether the patient may need escalation for imaging, surgical input, or a broader infection workup. The exam isn’t just descriptive. It’s a triage tool.
Common Causes and Clinical Implications
A tunneling wound usually signals that the visible opening is only part of the problem. In practice, I treat these wounds as evidence of deeper tissue failure, ongoing pressure, infection, poor perfusion, or a combination of those factors. The cause affects everything that follows, from dressing choice to whether home care is enough or a surgeon needs to be involved.
Where clinicians see tunneling most often
Tunneling is common in pressure injuries, diabetic foot ulcers, and some surgical wounds that break down after closure. It also shows up in patients with limited mobility, neuropathy, vascular disease, malnutrition, or a long inflammatory course. Those patterns matter at home as much as they do in clinic, because the daily forces that created the tunnel often continue between visits.
A patient who keeps sliding down in bed will keep generating shear. A person with diabetic neuropathy may keep walking on an unstable foot because pain is not giving useful warning. A post-operative wound with persistent drainage may be signaling deeper separation or bacterial burden rather than a simple surface problem.
Main drivers of tunnel formation
Several mechanisms repeatedly lead to tunneling wounds:
-
Pressure over time
Tissue near bone can break down below the surface before the skin opening looks dramatic. -
Shear
Sliding in bed, poor transfers, and prolonged positioning can pull tissue layers apart and create deeper injury. -
Infection or high bioburden
Bacteria and inflammatory debris can destroy tissue planes and extend the wound into a tract. -
Neuropathy and repeated trauma
Patients with reduced sensation may continue to bear weight or injure the area without realizing the damage is worsening. -
Poor blood flow
Ischemic tissue tolerates pressure and minor trauma badly, and it heals slowly once injured. -
Moisture imbalance and prolonged inflammation
Excess drainage, maceration, retained debris, and systemic factors can keep the wound from progressing in an orderly way.
A broader review of delayed wound healing causes helps explain why these wounds often persist unless both the local wound problem and the patient-level barriers are addressed.
Why the cause changes the clinical picture
The same tunnel can behave very differently depending on what is driving it.
A narrow tract in a diabetic foot ulcer raises concern for deeper extension, retained infection, and continued pressure with every step. A tunnel in a sacral pressure injury often reflects ongoing offloading failure, moisture exposure, or shear during repositioning. A tunneling surgical wound may point to fluid collection, dehiscence below the surface, or a local infection that needs more than routine dressing changes.
That is the practical gap families often run into. The wound may look small in the living room, but the decisions around it are not small. If the cause is still active at home, the tunnel usually persists.
Why untreated tunneling is dangerous
The main risk is hidden dead space. Fluid, debris, and bacteria can collect in that space and keep the wound from healing from the base upward. Some wounds stay deceptively unchanged for days, then deteriorate quickly once drainage is trapped or infection spreads.
Clinical consequences can include:
| Concern | Why it matters |
|---|---|
| Delayed healing | The tract prevents orderly filling with healthy tissue |
| Abscess or fluid collection | Closed spaces can trap drainage and promote infection |
| Progressive tissue destruction | Damage may extend beyond what is visible at the skin |
| Cellulitis or deeper infection | Local infection can spread into surrounding tissue or deeper structures |
For caregivers and primary care teams, the implication is straightforward. A tunneling wound is not a routine surface wound needing a bandage changed on schedule. It needs the cause identified, pressure and shear reduced at home, drainage watched closely, and a clear plan for when worsening drainage, odor, pain, fever, redness, or sudden depth changes should trigger urgent reassessment.
Advanced Treatment and Management Strategies
A tunneling wound rarely improves with a surface dressing alone. The tract has to be assessed, cleaned when appropriate, and managed in a way that supports healing from the deepest point outward. That is the difference between a plan that looks reasonable on paper and one that is effective in the home.
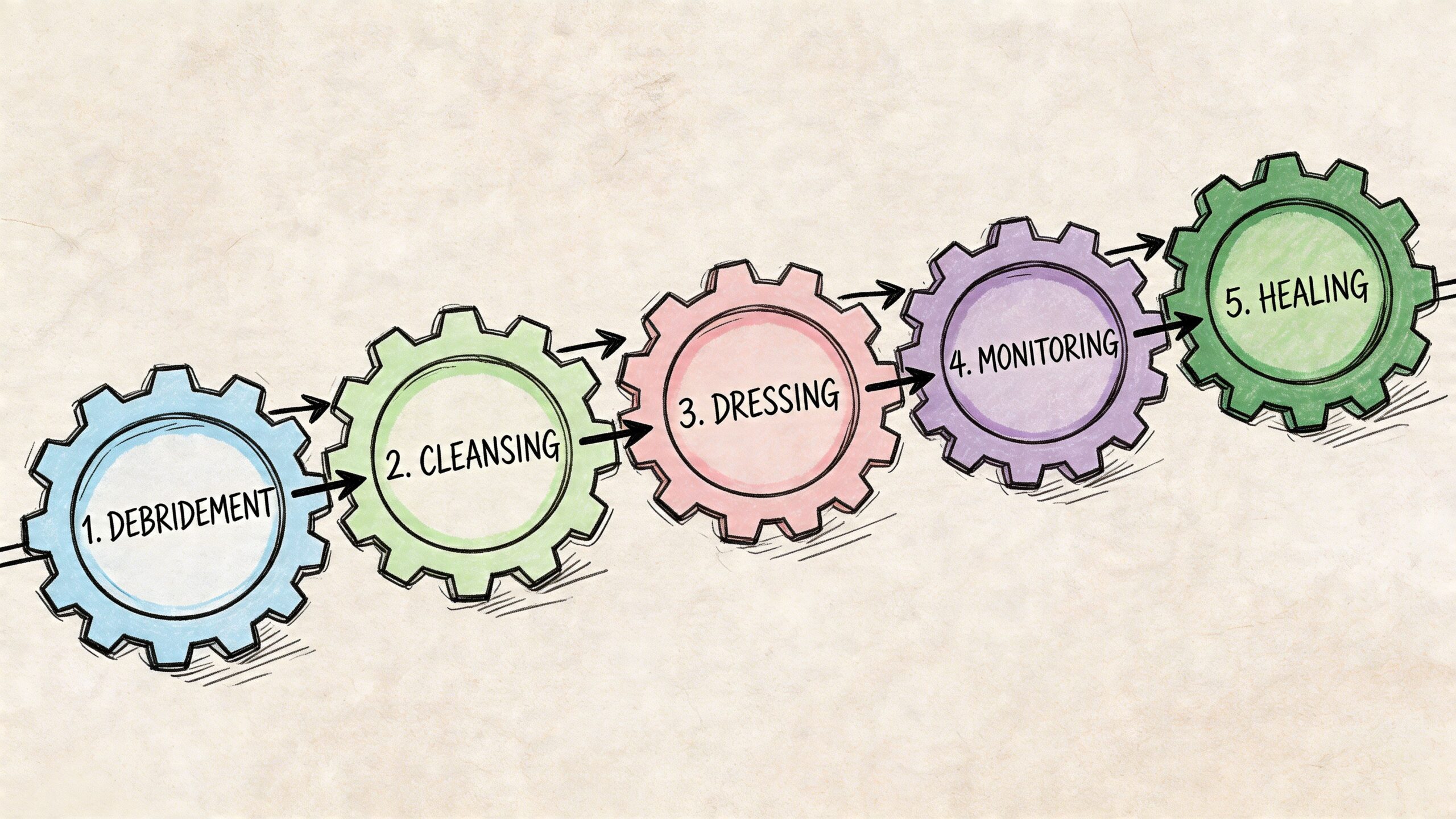
Debridement comes first when nonviable tissue is present
If slough, necrotic tissue, or infected debris extends into the tunnel, the wound often stalls until that material is removed. Debridement lowers bioburden and exposes healthier tissue that can support granulation.
There is a real trade-off here. Conservative care may feel safer to families who are worried about pain or bleeding, but retained nonviable tissue can keep inflammation active and trap drainage. Aggressive debridement has its own risks if the clinician cannot clearly distinguish dead tissue from viable structures. The method has to match the wound, the blood supply, the pain level, and the care setting.
Packing has to match the wound, not the habit
Packing should fill dead space lightly enough to avoid pressure injury and fully enough to prevent the tract from sealing over the top while deeper space remains open. In practice, that means the material, amount, and direction of placement matter.
Underpacking can allow fluid to collect. Overpacking can compress fragile tissue and delay granulation. Ribbon gauze, alginate, hydrofiber, or other packing materials may be appropriate depending on drainage, tissue condition, and whether the wound can be safely re-explored at the next dressing change. Every piece placed into a tunnel must also be removable in full. Retained packing is a preventable cause of infection and delayed healing.
Incorrect packing keeps many tunneling wounds from progressing. The goal is support, drainage control, and safe healing from the base upward.
Negative pressure therapy can help selected wounds
For the right patient, negative pressure wound therapy alters the wound environment in ways standard dressings cannot. It can improve exudate control, help draw wound edges together, and support granulation tissue in a larger cavity or complex wound with tunneling.
It is not automatic treatment for every tunnel. A wound with untreated necrosis, uncontrolled infection, unexplored depth, active bleeding risk, or exposed structures may need a different first step. In home care, success also depends on practical factors such as seal integrity, caregiver comfort with the device, and how often the dressing will need to be changed. A technically good therapy fails quickly if the dressing cannot stay in place in the patient’s living room.
The body must also move out of a state of chronic inflammation for healing to progress. A review in Advances in Wound Care describes how persistent inflammation and excess protease activity can impair healing in chronic wounds, which is why treatment often extends beyond local dressings to correcting edema, improving nutrition, and addressing the underlying cause of tissue injury, as reviewed in this PubMed-indexed article on chronic wound pathophysiology and treatment approaches.
Treatment works best in a clinical sequence
Advanced wound care is usually a sequence of decisions rather than a list of products. The team has to determine what is blocking progress first, then choose the next intervention with that obstacle in mind.
Typical questions include:
- Is infection present, or is drainage collecting in a way that needs urgent source control?
- Does the wound need debridement before dressings or advanced therapies will be effective?
- Is the tunnel being packed correctly for its depth, direction, and drainage level?
- Would negative pressure therapy improve exudate management and tissue formation in this case?
- Can the current plan be carried out reliably at home, with clear instructions for dressing changes and warning signs?
What tends to slow progress
Several patterns repeatedly interfere with healing:
- Using a surface-only dressing for a wound with meaningful depth or dead space
- Letting the tract dry out when the wound needs moisture balance for cell activity
- Packing by routine instead of by measurement, especially when the tunnel depth is changing
- Ignoring edema, pressure, shear, or glucose control
- Switching products too often without reassessing the wound bed, tunnel direction, and cause
- Spacing follow-up too far apart for a wound that needs serial measurement and plan adjustment
As the tunnel fills with healthier tissue and drainage decreases, the dressing strategy should change with it. Good management is active, measured, and practical enough to hold up between clinic visits.
The Critical Role of Supportive Care
Even the best debridement and dressing plan will underperform if the patient keeps loading pressure onto the wound, sits in unrelieved edema, or doesn’t have the nutritional reserve to build tissue. Supportive care is where many outcomes are won or lost.
Offloading isn’t optional
For pressure injuries and diabetic foot ulcers, offloading is part of treatment, not an extra instruction at the end of the visit. If the wound is on the heel, sacrum, or plantar foot, each hour of ongoing pressure works against the dressing and the tissue response.
That often means changing bed positioning, transfer technique, footwear, seating surfaces, or walking patterns. In home care, caregivers become essential. They see the daily habits that either protect the wound or keep reopening it.
Compression and edema control
If venous disease is part of the picture, edema control matters. A beautifully chosen dressing won’t compensate for uncontrolled swelling. When the leg remains edematous, tissue oxygenation, drainage handling, and skin integrity all suffer.
That’s why clinicians often combine local wound care with medical-grade compression therapy when the vascular picture supports it. The wrap or compression system isn’t separate from wound treatment. It is wound treatment for the right patient.
A tunneling wound closes more reliably when the care plan treats the cause beneath it, not just the opening above it.
Nutrition, medications, and the whole patient
The body needs protein, calories, micronutrients, and adequate hydration to build granulation tissue and remodel collagen. If a patient is eating poorly, losing weight, dealing with nausea, or living with catabolic illness, wound progress usually reflects that.
Supportive review should also include medications and risk factors that interfere with repair. Some patients need tighter coordination between wound care, primary care, podiatry, vascular care, and home health. That coordination is often what separates temporary improvement from durable healing.
Home Care Guidance and Red Flags for Caregivers
Most wound care happens between visits. Families and caregivers don’t need to perform specialist-level assessment, but they do need to protect the treatment plan and recognize when the wound is changing in a concerning way.
What to do at home
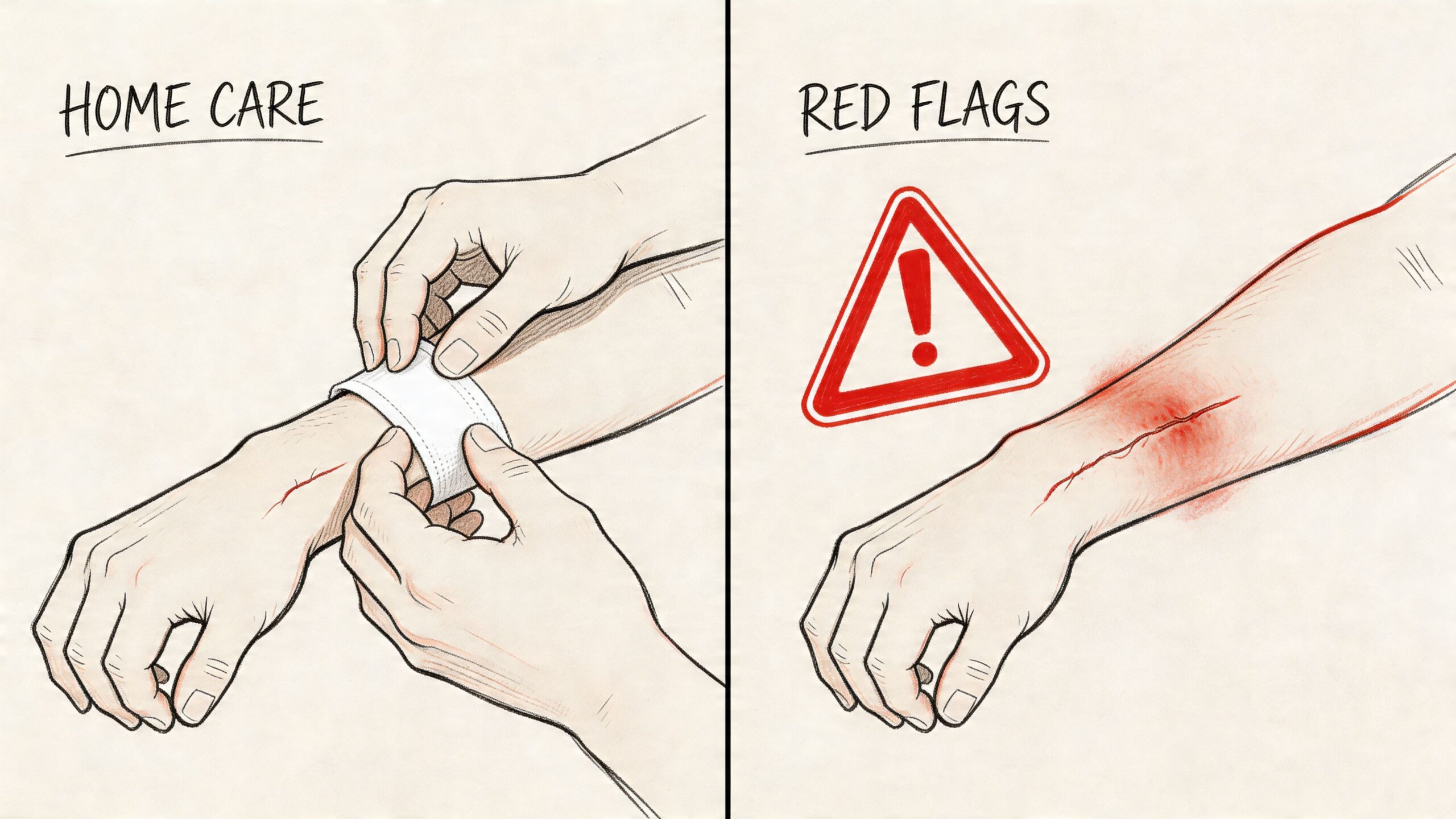
Keep home care simple and consistent:
- Protect the dressing: Keep it clean, dry, and in place unless your clinician gave different instructions.
- Follow the exact change schedule: Early removal, delayed changes, or substitute supplies can disrupt progress.
- Reduce pressure: Reposition as instructed. Don’t sit or lie on the wound if that area is supposed to be offloaded.
- Watch the drainage: Not every change is an emergency, but changes should be noticed and reported.
- Bring questions forward early: If dressing changes become difficult, painful, or confusing, the plan may need adjustment.
A short visual review can help caregivers understand basic wound warning signs and dressing awareness:
Red flags that need a call
Call the wound team promptly if you notice any of the following:
- New or increasing pain: Especially if the wound had been relatively stable
- Foul odor: A stronger or new odor can signal tissue breakdown or infection
- Drainage changes: More drainage, thicker drainage, or a change in color
- Spreading redness or warmth: Particularly around the wound edge or beyond it
- Fever or sudden decline: Weakness, confusion, or feeling acutely unwell needs attention
Don’t wait for the next scheduled visit if the wound suddenly looks or smells different, or if the patient seems systemically worse.
What caregivers should avoid
Don’t probe the wound at home. Don’t push packing farther into a tract unless you’ve been specifically trained to do that task. Don’t use random over-the-counter products because they “worked before” on a different wound. Tunneling wounds punish guesswork.
When to See a Specialist The Windy City Wound Care Advantage
A tunneling wound needs more than routine skin care. It needs clinical assessment of depth and direction, ongoing measurement, and a treatment plan that addresses infection risk, dead space, pressure, circulation, and the patient’s overall healing capacity.
That’s especially important when the patient is older, has diabetes, limited mobility, venous disease, or a wound that hasn’t improved with standard care. The practical barrier, of course, is that many of these patients have the hardest time getting to a wound clinic. Travel is painful, transfers are difficult, and delays are common when care depends on transportation.
That’s where mobile specialty care makes a real difference. Windy City Wound Care brings advanced wound treatment directly to patients in the home, assisted living, and skilled nursing settings across the Chicago area. That model makes it easier to assess the wound in the setting where pressure, transfers, footwear, bedding, and caregiver routines affect healing.
For patients, families, discharge planners, primary care teams, podiatrists, and facility staff, early referral is the safest move when a wound appears deeper than expected, stalls, drains persistently, or shows signs of tunnel formation. Fast specialist involvement often prevents a much bigger problem later.
If you’re dealing with a wound that seems deeper than it looks, Windy City Wound Care can help evaluate it in the setting where day-to-day care happens. Their mobile clinicians provide advanced wound assessment and treatment across Chicago and surrounding Illinois counties, including care in private homes, assisted living communities, and skilled nursing facilities. To request a consultation, call 708-497-9850. Referring providers can fax referrals to 844-333-1773.
