A patient notices that one leg has been swelling for months. By evening, the ankle feels tight, the skin looks darker, and walking is uncomfortable. Another patient has persistent fullness in the foot and toes that doesn’t change much with rest, even when the leg is raised. Both say the same thing: “My leg is swollen.” Clinically, those are not the same problem.
That’s where confusion starts. In practice, chronic venous insufficiency vs lymphedema is one of the most important distinctions to make early, because the wrong label leads to the wrong treatment plan, and delayed treatment is how edema turns into skin breakdown, recurrent cellulitis, and chronic wounds.
For referring physicians, caregivers, and informed patients, the key isn’t memorizing terminology. It’s recognizing patterns. Venous disease is a failure of blood return. Lymphedema is a failure of lymphatic drainage. Some patients have one. Some have the other. Some have both, and that overlap is often missed until the swelling becomes fixed and the skin becomes hard, fibrotic, or ulcerated.
Decoding the Cause of Your Chronic Leg Swelling
A common referral starts with a vague description: leg swelling, heaviness, redness, maybe a draining wound near the ankle. The patient may already have tried over-the-counter compression socks, occasional elevation, a topical cream, or a course of antibiotics. The swelling improves a little, then returns. That pattern should raise suspicion that the issue hasn’t been correctly classified.

In wound care, the distinction matters because the tissue tells the story over time. Venous disease often announces itself with ankle-predominant edema, aching with prolonged standing, hyperpigmentation, and wounds near the gaiter region. Lymphedema behaves differently. The swelling is often more persistent, may involve the foot and toes more clearly, and tends not to respond the way venous edema does.
Why patients and clinicians get this wrong
The first problem is that both conditions cause visible swelling.
The second is that both can produce skin change, discomfort, mobility loss, and eventually ulcer risk. Once chronic inflammation sets in, bedside impressions become less reliable unless you step back and ask the right questions about timing, symmetry, location, and response to elevation.
The practical question to ask first
Don’t start with, “What is the diagnosis?” Start with, “What system is failing?”
- If venous return is failing, blood pools in the lower extremity.
- If lymphatic drainage is failing, protein-rich fluid remains trapped in tissue.
- If both systems are failing, the patient may have a mixed picture that won’t improve with a single-track plan.
Swelling that keeps recurring despite partial treatment usually means the original diagnosis was incomplete, not that the patient “failed” care.
That’s the clinical frame that improves outcomes. Once you identify whether the problem is venous, lymphatic, or combined, treatment becomes more precise, compression becomes more intentional, and wound prevention becomes more realistic.
Understanding the Two Systems Behind Swelling
Edema in the lower extremity usually comes from one of two transport systems not doing their job. One returns blood to the heart. The other clears interstitial fluid and proteins from the tissues. They work together, but they fail in different ways.
Chronic venous insufficiency
Chronic venous insufficiency, or CVI, develops when leg vein valves don’t maintain effective one-way flow. Blood refluxes and pools distally. That raises venous pressure in the lower extremity and drives fluid into surrounding tissues.
Clinically, that means patients often report worsening symptoms over the course of the day, especially with prolonged standing or walking. The edema typically centers around the ankles and lower legs. Discomfort is usually described as aching, heaviness, or cramping rather than simple “swelling.”
CVI is also common. A review in the National Library of Medicine reports that CVI affects 25% to 40% of adult females and 10% to 20% of adult males globally and notes that prolonged venous hypertension can overwhelm the lymphatic system and produce secondary lymphedema, often called phlebolymphedema, in advanced disease (review of chronic venous insufficiency and lymphatic involvement).
Lymphedema
Lymphedema is different at the mechanism level. The lymphatic system isn’t clearing fluid and proteins effectively, so tissue fluid accumulates and gradually changes the character of the skin and subcutaneous tissue.
The cause may be primary, from congenital lymphatic abnormality, or secondary, after surgery, radiation, trauma, infection, inflammation, obesity, or other structural disruption. The visible result is often fuller, more persistent swelling that may involve the foot and toes and may not improve much with simple positioning.
Why the distinction changes management
These aren’t two names for the same thing.
- CVI treatment goal: improve venous return and control venous hypertension.
- Lymphedema treatment goal: support lymphatic drainage and long-term volume control.
- Mixed disease goal: address both systems before tissue damage becomes fixed.
Clinical shortcut: CVI is a pressure and reflux problem. Lymphedema is a drainage and transport problem.
That distinction explains why some patients improve with standard venous compression and leg elevation, while others don’t. It also explains why a patient can start with venous edema and later present with a more complex picture that no longer behaves like uncomplicated CVI.
A Side-by-Side Comparison of Key Clinical Signs
A common referral pattern goes like this. The patient has chronic lower-leg swelling, compression helped at first, and now the foot is enlarging, the skin is firmer, and the edema no longer behaves like straightforward venous disease. That shift should raise suspicion for lymphatic involvement, especially phlebolymphedema rather than isolated CVI.
Quick clinical comparison
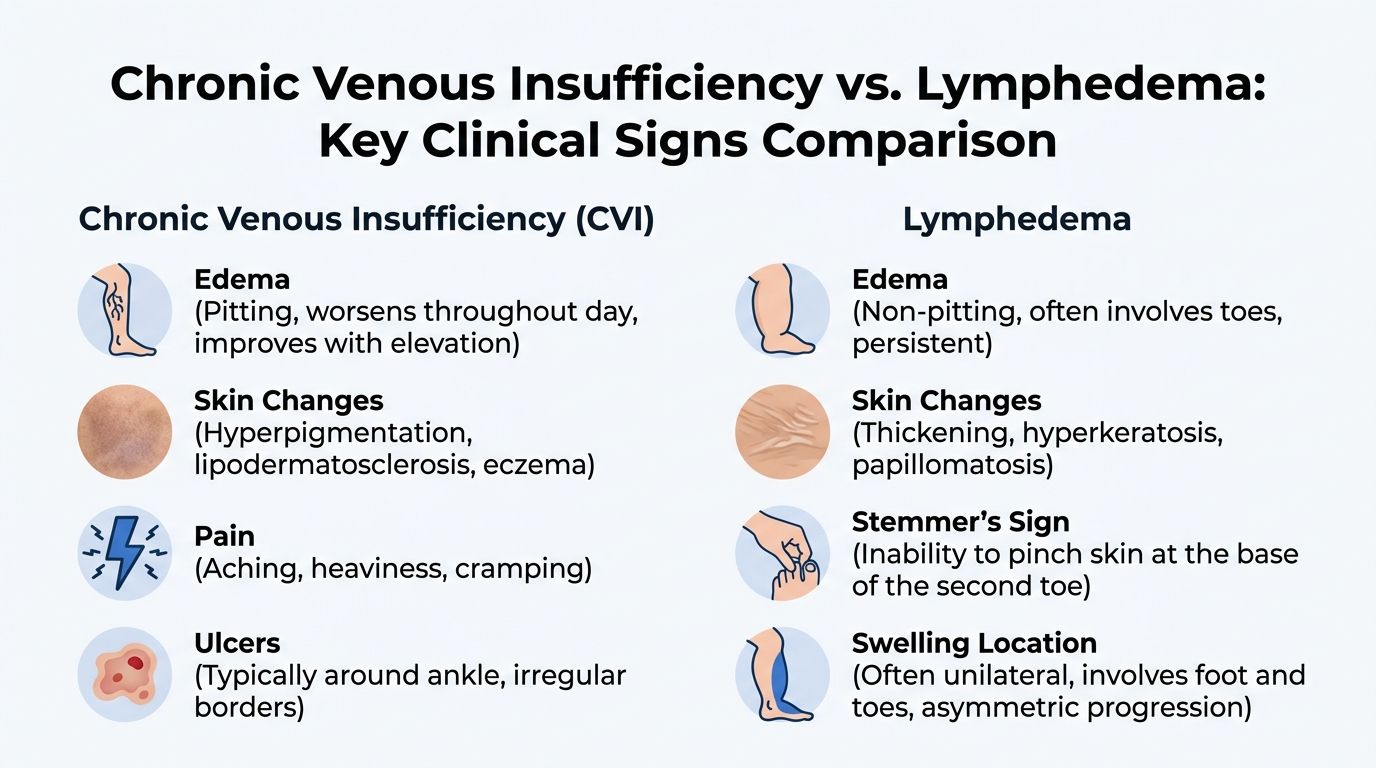
| Feature | Chronic Venous Insufficiency (CVI) | Lymphedema |
|---|---|---|
| Typical cause | Venous valve failure with blood pooling | Lymphatic drainage failure |
| Usual distribution | Lower legs and ankles, often below the knee | May involve the entire limb, foot, and toes |
| Symmetry | Commonly bilateral and relatively symmetric | Often asymmetric or unilateral |
| Effect of standing | Usually worsens | May remain persistently swollen regardless of position |
| Effect of elevation | Often improves | Often changes little |
| Sensation | Aching, heaviness, cramping | Fullness, heaviness, limb bulk |
| Skin findings | Hyperpigmentation, venous dermatitis, lipodermatosclerosis, varicose veins | Thickening, hyperkeratosis, papillomatous change |
| Ulcer pattern | More consistent with venous ulcers near the ankle region | Less typical as a primary ulcer pattern without another driver |
| Foot and toe involvement | Less dominant early clue | Often important clinically |
Patterns that matter more than any single symptom
Single findings mislead. The whole limb pattern is what separates venous edema from lymphatic edema, and it is often what exposes mixed disease.
Start with distribution. CVI usually declares itself at the gaiter area, ankle, and lower calf. Lymphedema more often includes the dorsum of the foot and the toes. Once the foot is clearly involved, especially with squaring of the toes or dorsal fullness, I become more concerned that the lymphatic system is no longer keeping up.
Then assess tissue quality. Venous disease tends to produce stasis pigmentation, dermatitis, varicosities, and lipodermatosclerosis. Lymphedema produces denser tissue, progressive skin thickening, hyperkeratosis, and in later cases a more fibrotic feel that does not pit the same way as early edema.
Symmetry helps, but only in context. Bilateral swelling fits CVI more often, yet bilateral disease does not rule out lymphedema, particularly in obese patients or those with long-standing venous hypertension. Marked asymmetry should widen the differential and prompt a closer exam for prior surgery, trauma, malignancy treatment, recurrent cellulitis, or unilateral venous obstruction.
Pain description also matters. Patients with CVI often report aching or pressure that builds with dependency. Patients with lymphedema usually describe heaviness, tightness, or limb bulk. In phlebolymphedema, they often report both. That mixed symptom pattern is one reason online side-by-side checklists miss the diagnosis.
A bedside Stemmer-type sign can help when toe involvement is present and the skin is thickened. It is supportive, not definitive. The more useful question is whether the exam still fits uncomplicated venous disease, or whether chronic venous overload has started to produce secondary lymphatic failure.
If there is skin breakdown, drainage, or a chronic ulcer, the swelling pattern has to be interpreted alongside the wound exam. A structured wound assessment for drainage, tissue quality, and periwound skin changes often clarifies whether venous hypertension alone explains the presentation or whether lymphatic congestion is contributing to delayed healing.
The most dependable diagnosis comes from the distribution of swelling, the skin changes, and the tissue texture taken together. That is also how phlebolymphedema stops being missed.
Navigating the Diagnostic Pathway
A correct diagnosis comes from combining history, exam, and targeted imaging. Swelling alone doesn’t justify a one-size-fits-all compression plan.
History and bedside clues
Start with simple but discriminating questions.
- What makes the swelling better or worse? Venous edema usually improves with elevation and worsens with dependency.
- Where did the swelling begin? Ankle-predominant swelling behaves differently from foot-and-toe swelling.
- How fast did it appear? Gradual progression in an older patient suggests one pathway. Post-surgical or post-traumatic onset suggests another.
- Is there a wound, drainage, or recurrent cellulitis? That changes urgency and broadens the differential.
One useful bedside benchmark is response to elevation. A vascular center summary notes that CVI swelling typically reduces after 20 to 30 minutes of elevation, whereas lymphedema fluid remains largely unchanged because the lymph-rich fluid is trapped within tissues (diagnostic clue based on limb elevation response).
If you’re evaluating concurrent skin breakdown, this guide on how to assess a wound is useful because wound location, drainage pattern, edge quality, and periwound skin often reinforce the underlying edema diagnosis.
Imaging that changes management
The next step is choosing imaging that answers the clinical question.
For suspected venous disease, venous duplex ultrasound is the key study. It evaluates reflux, obstruction, and overall venous anatomy. If reflux is present in the expected clinical setting, the edema has a venous driver even if skin changes are already advanced.
For suspected lymphatic disease, lymphoscintigraphy is the more specific study when the diagnosis remains uncertain after clinical evaluation. It helps identify lymphatic transport failure and can clarify whether the persistent edema is lymphatic, venous, or mixed.
A short visual review can help patients and families understand why the workup differs between these disorders:
Don’t assume all chronic leg edema is venous because the patient is older, or lymphatic because the foot is swollen. Confirm the dominant mechanism before escalating treatment.
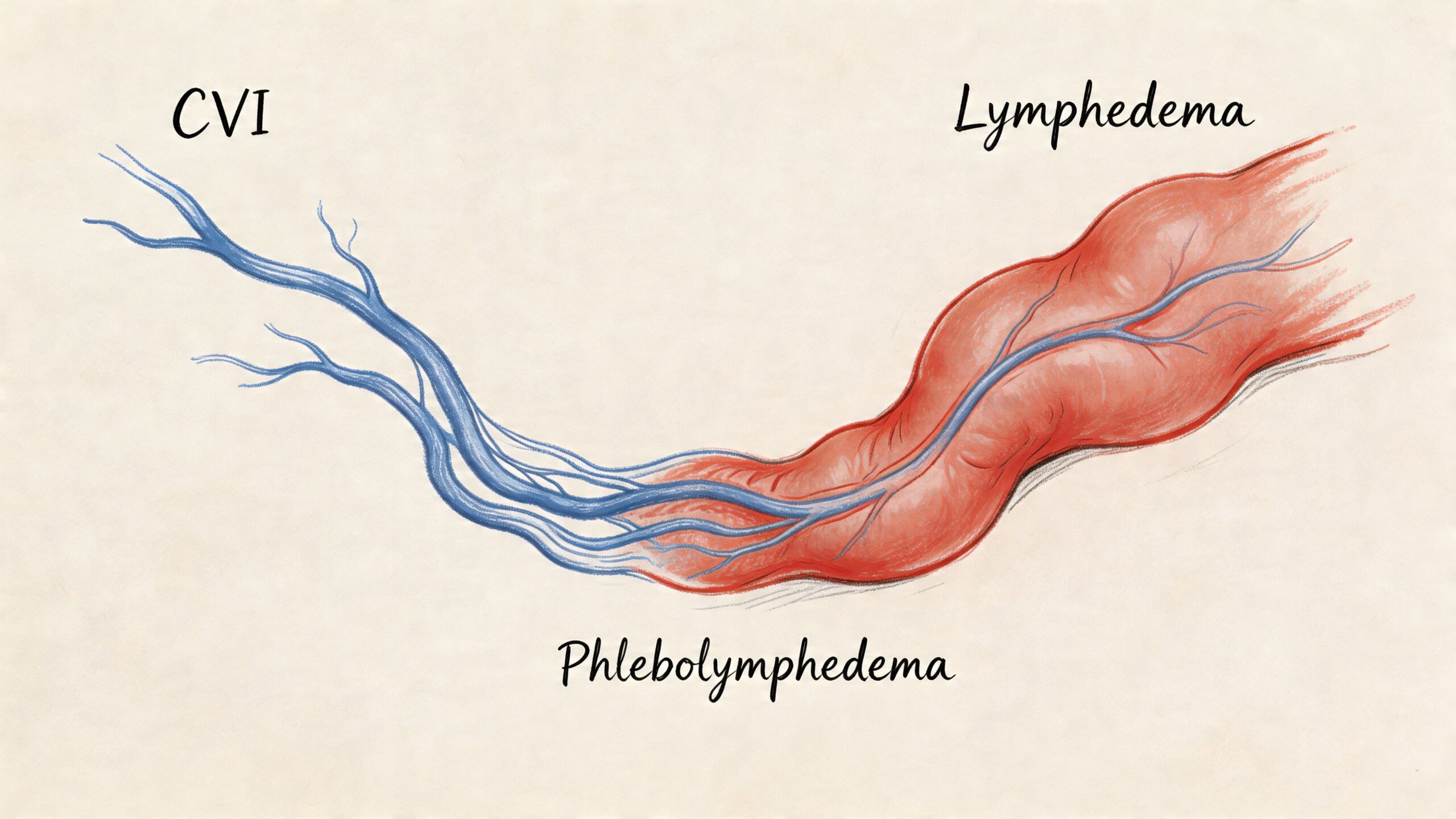
Identifying Phlebolymphedema The Critical Overlap
The most overlooked diagnosis in chronic venous insufficiency vs lymphedema discussions is the patient who has stopped fitting cleanly into either category. That patient may have phlebolymphedema.
When venous disease stops being purely venous
In long-standing venous hypertension, the lymphatic system has to carry more fluid load for more time. Eventually it can’t keep up. Then it begins to fail structurally and functionally.
The result is not just more edema. The result is a change in edema behavior. Swelling becomes less reversible, less responsive to elevation, more fibrotic, and more clinically stubborn.
A monograph from the Lymphatic Education & Research Network describes phlebolymphedema as a critical venolymphatic failure where chronic venous hypertension overwhelms lymphatic capacity, and notes that imaging can separate the components, with lymphoscintigraphy showing dermal backflow in lymphedema while venous duplex identifies reflux or obliteration in CVI (monograph on phlebolymphedema and venolymphatic failure).
Why this matters in wound care
This overlap matters because mixed disease often explains treatment disappointment.
A patient may undergo venous intervention and still have persistent leg volume. Another may receive generic compression without a structured lymphatic plan and continue progressing toward skin thickening and ulceration. Neither scenario means treatment was useless. It means the disease was incompletely framed.
Common clues that suggest phlebolymphedema include:
- Swelling that once improved but no longer does
- Venous skin changes plus increasing foot or toe involvement
- Ulcer history with persistent limb bulk after venous treatment
- Fibrotic or woody tissue that makes standard compression harder to apply effectively
A patient with venous disease and fixed edema shouldn’t be labeled “refractory” until you’ve considered secondary lymphatic failure.
In practice, this is the group that benefits most from coordinated venous and lymphatic planning rather than a single-discipline approach.
Contrasting Individualized Treatment and Management Plans
Treatment only works when it matches the mechanism. That sounds obvious, yet many chronic edema patients lose months of progress precisely because of this.
What works for CVI
For CVI, the main targets are venous hypertension control, edema reduction, skin protection, and ulcer prevention or healing.
That usually means:
- Compression with a venous goal: enough structure to support venous return and reduce dependent edema
- Elevation and calf pump activation: useful because venous edema is position-sensitive
- Skin surveillance: especially when dermatitis, hyperpigmentation, or fragile periwound tissue is present
- Ulcer-directed care when wounds are present: debridement when indicated, moisture balance, infection control, and protection of the surrounding skin
For patients with venous leg ulcers, treatment fails when clinicians focus only on the wound bed and ignore the edema driver. Dressings alone won’t overcome uncontrolled venous hypertension.
What works for lymphedema
Lymphedema management has a different center of gravity. The issue isn’t just pressure control. It’s volume management over time.
This plan often includes:
- Lymphatic-focused compression systems
- Manual techniques and decongestive strategies when appropriate
- Meticulous skin care
- Garment selection that patients can apply and maintain
- Long-term maintenance rather than intermittent treatment
Lymphedema also punishes inconsistency. A technically good plan that the patient can’t manage at home won’t hold.
What fails in mixed disease
Phlebolymphedema is where rigid treatment silos break down. A venous-only plan may leave residual limb volume. A lymphatic-only plan may under-address reflux and ulcer risk.
A vein practice review points out that many online comparisons underaddress phlebolymphedema, despite the need for integrated care that combines venous procedures with lymphatic therapies to prevent non-healing wounds (discussion of the phlebolymphedema treatment gap).
That integrated approach is often best delivered where the patient lives, especially when mobility, pain, or wound burden makes repeated office travel unrealistic. Services such as compression therapy at home can support ongoing edema control, reassessment of fit and tolerance, and closer observation of skin and wound response in real-world conditions.
A practical management rule:
- If swelling improves quickly with elevation, think venous-dominant
- If swelling persists with foot involvement and tissue thickening, think lymphatic involvement
- If venous signs and persistent edema coexist, treat the overlap, not the label
Management principle: Don’t ask whether compression is indicated. Ask what kind, for what goal, and under whose follow-up.
When to Refer for Specialist Wound Care
Referral should happen before edema becomes a chronic wound problem, not after months of stalled healing.
Send the patient for specialist wound evaluation when any of the following are present:
- A non-healing lower leg wound: especially around the ankle or in chronically swollen tissue
- Recurrent cellulitis or increasing drainage: these patients often have more than simple edema
- Hard, woody, or fibrotic skin: that usually signals more advanced tissue change
- Rapid decline in mobility: because swelling control becomes much harder once activity drops
- Repeated treatment failure: including persistent swelling after vein treatment or compression that isn’t holding
For referring clinicians, this is often the point where chronic edema and wound management need to happen together. Venous ulcers, pressure injuries in edematous limbs, and diabetic foot wounds all get harder to manage when limb volume is uncontrolled.
If a wound has stalled, this article on why a leg ulcer may not be healing is a useful checkpoint because edema, bioburden, and incorrect compression plans commonly coexist.
The practical reason to refer early is simple. Once skin breaks down in an edematous limb, every delay makes dressing selection, compression tolerance, infection control, and caregiver adherence more difficult.
Frequently Asked Clinical Questions
Can a patient have both CVI and lymphedema
Yes. In practice, this overlap is common, and it is often missed until swelling stops responding to a vein-focused plan alone.
A typical pattern starts with chronic venous insufficiency, then prolonged venous hypertension overloads the lymphatic system and secondary lymphedema develops. That combined condition is phlebolymphedema. It explains why a patient may still have heavy, persistent limb swelling after venous treatment, or why compression that once worked no longer controls limb volume.
The reverse also occurs. A patient with underlying lymphatic dysfunction can develop venous disease that adds ankle skin change, pain, and wound risk.
Is there a cure or is this long-term management
For both conditions, treatment usually means long-term control rather than a one-time fix.
The clinical goals are clear. Reduce limb volume. Protect the skin barrier. Prevent cellulitis and ulceration. Maintain walking, shoe fit, and tolerance of compression. In phlebolymphedema, management usually needs more than one tool because treating the venous component without addressing lymphatic failure leaves part of the problem in place.
Good plans are realistic enough to follow outside the clinic.
Which specialist should evaluate chronic leg swelling
The right referral depends on what is driving the swelling and whether tissue injury is already present.
Venous-predominant disease may need vascular evaluation. Suspected lymphedema often benefits from a certified lymphedema therapist. Mixed swelling, recurrent cellulitis, drainage, fibrosis, or ulceration usually needs a coordinated plan that includes wound care early, especially when phlebolymphedema is on the differential.
A practical rule helps. If the edema pattern no longer fits a single-system diagnosis, or treatment aimed at one system has stalled, reassess for overlap rather than repeating the same plan.
What findings make phlebolymphedema more likely
Look for combined signs.
Patients may have venous clues such as gaiter-area discoloration, varicosities, or a history of venous ulcer, along with lymphatic features such as foot or toe involvement, thickened tissue, squaring of the toes, or swelling that becomes less pitting over time. That mixed presentation matters because it usually changes compression selection, skin care intensity, and follow-up needs.
Can compression help both conditions
Often yes, but the prescription has to match the limb.
A patient with CVI may do well with standard graduated compression if arterial inflow is adequate and the limb shape allows it. Lymphedema, especially with fibrosis or foot involvement, may need a different approach such as short-stretch wraps, layered bandaging, or adjustable compression garments. In phlebolymphedema, poor garment fit, pain, rolling, or persistent forefoot swelling are common reasons standard stockings fail.
What is the main takeaway for patients and referring clinicians
Use the pattern of swelling to guide the next step.
- Ankle-predominant edema with skin staining or venous ulcer history points toward venous disease
- Foot and toe involvement, progressive tissue thickening, or recurrent cellulitis points toward lymphatic disease
- Features of both should raise concern for phlebolymphedema
If chronic leg swelling is contributing to delayed healing, recurrent skin injury, cellulitis, or difficulty maintaining compression, Windy City Wound Care provides mobile advanced wound care in the home, assisted living, and skilled nursing settings across the Chicago area. Referring clinicians, caregivers, and patients can request an evaluation when edema control and wound management need to happen together.

