A slow-to-heal wound changes the rhythm of daily life fast. Dressing changes start to dictate the day. Walking becomes guarded. Sleep gets interrupted. Family members begin watching the wound almost as closely as the patient does, wondering why it still looks inflamed, wet, painful, or unchanged after weeks of treatment.
That pattern is common with diabetic foot ulcers, venous leg ulcers, pressure injuries, and post-surgical wounds that stall in a setting of edema, poor perfusion, pressure, friction, or bacterial burden. Standard care still matters. Offloading, compression, moisture balance, debridement, infection control, and nutrition remain the foundation. But some wounds don’t move forward with basic treatment alone. If you’re dealing with a wound that seems stuck, understanding the common causes of delayed wound healing can clarify why progress has slowed.
Mist therapy for wounds is one of the advanced tools used when a wound needs more than routine care. It isn’t a shortcut, and it isn’t a replacement for sound wound management. It is a targeted modality that can help clean the wound environment and stimulate healing in selected patients, especially when traditional debridement is poorly tolerated or the wound bed remains chronically stagnant.
The Challenge of Slow-to-Heal Wounds
A wound can look “small” and still be clinically serious. I see this most often with neuropathic foot ulcers that don’t hurt enough to keep a patient off the area, venous ulcers that remain inflamed because edema control isn’t consistent, and pressure injuries in patients who can’t reposition well on their own. The visible opening is only part of the problem. The larger issue is often the wound environment beneath the surface.
Why standard care sometimes stalls
A wound usually stops progressing for a reason, not by chance. Common drivers include:
- Persistent bioburden: The wound may look cleaner after a dressing change but still carry enough bacterial burden or biofilm to interfere with granulation.
- Poor tolerance for debridement: Some patients can’t comfortably tolerate sharp debridement, or the wound location makes aggressive bedside debridement impractical.
- Mechanical obstacles: Pressure, shear, and edema keep undoing any gains made during treatment.
- Fragile host factors: Diabetes, vascular disease, limited mobility, and advanced age all complicate the healing response.
When that happens, escalating care isn’t “doing more for the sake of more.” It’s matching the treatment to the wound’s behavior.
Slow progress is still clinical information. A wound that isn’t shrinking, cleaning up, or building granulation is telling you the current plan isn’t enough.
Where mist therapy fits
Mist therapy for wounds is best understood as an adjunct within a larger wound plan. It can help with wound bed preparation, especially when the tissue is stalled, sensitive, or difficult to debride conventionally. In home-based care, that’s especially useful because many patients need effective treatment that doesn’t depend on repeated travel to a clinic or operating room.
The practical value is straightforward. If a wound can be cleaned more gently, stimulated more consistently, and treated where the patient lives, adherence usually improves and disruption drops.
How Mist Therapy Accelerates Wound Healing
Mist therapy uses low-frequency, non-contact ultrasound delivered through saline mist. In practice, that means the wound can be treated without dragging a curette, gauze, or other instrument across tissue that is already painful, friable, or prone to bleeding.
For home-bound patients, that difference is often meaningful. A treatment that is easier to tolerate is easier to complete consistently, and consistency matters in chronic wound care.
A visual summary helps make the mechanism clearer.

What it’s doing at the wound surface
At the wound surface, mist therapy is used to improve wound bed conditions. The saline mist carries the ultrasound energy to the tissue, which helps loosen nonviable material, disrupt biofilm, and reduce surface contamination without direct contact. That can be useful in wounds that remain inflamed despite appropriate dressings and routine care.
The non-contact approach has a practical advantage in mobile wound care. Heel ulcers, sacral pressure injuries, and painful lower extremity wounds can be difficult to treat aggressively in the home if the patient cannot tolerate repeated sharp debridement. Mist therapy does not replace debridement when debridement is required, but it can make wound bed preparation more manageable between visits and in patients with limited tolerance.
What it’s doing below the surface
Mist therapy is also used for its biologic effects. Clinical discussions of non-contact low-frequency ultrasound describe effects on local circulation and cellular activity involved in repair. In practical terms, the goal is not only to clear barriers at the surface, but to encourage granulation and a more active healing response in tissue that has stalled.
That distinction matters in real-world care. Some treatments mainly protect the wound. Others mainly remove debris. Mist therapy is useful because it can support both tissue preparation and tissue response when the rest of the plan is sound.
Expectations need to stay realistic. If edema is uncontrolled, offloading is inconsistent, perfusion is poor, or blood glucose remains high, ultrasound will not overcome those factors. It works best as part of an evidence-based wound care plan that addresses the reason the wound stalled in the first place.
That is also where the mobile model matters. At Windy City Wound Care, treatment is delivered where the patient lives, so clinicians can pair mist therapy with hands-on assessment of adherence barriers, dressing technique, pressure relief, edema control, and caregiver support. For many patients, especially those covered under Medicare Part B who have difficulty traveling, that practical setup affects whether an advanced therapy is merely ordered or completed.
For patients who want to see the device and treatment setup in action, this overview is helpful.
The Clinical Evidence for Mist Therapy
Clinical evidence matters because chronic wounds can appear stable while making very little real progress. In practice, the question is simple. Does adding noncontact low-frequency ultrasound improve healing outcomes enough to justify the added visits, documentation, and cost?
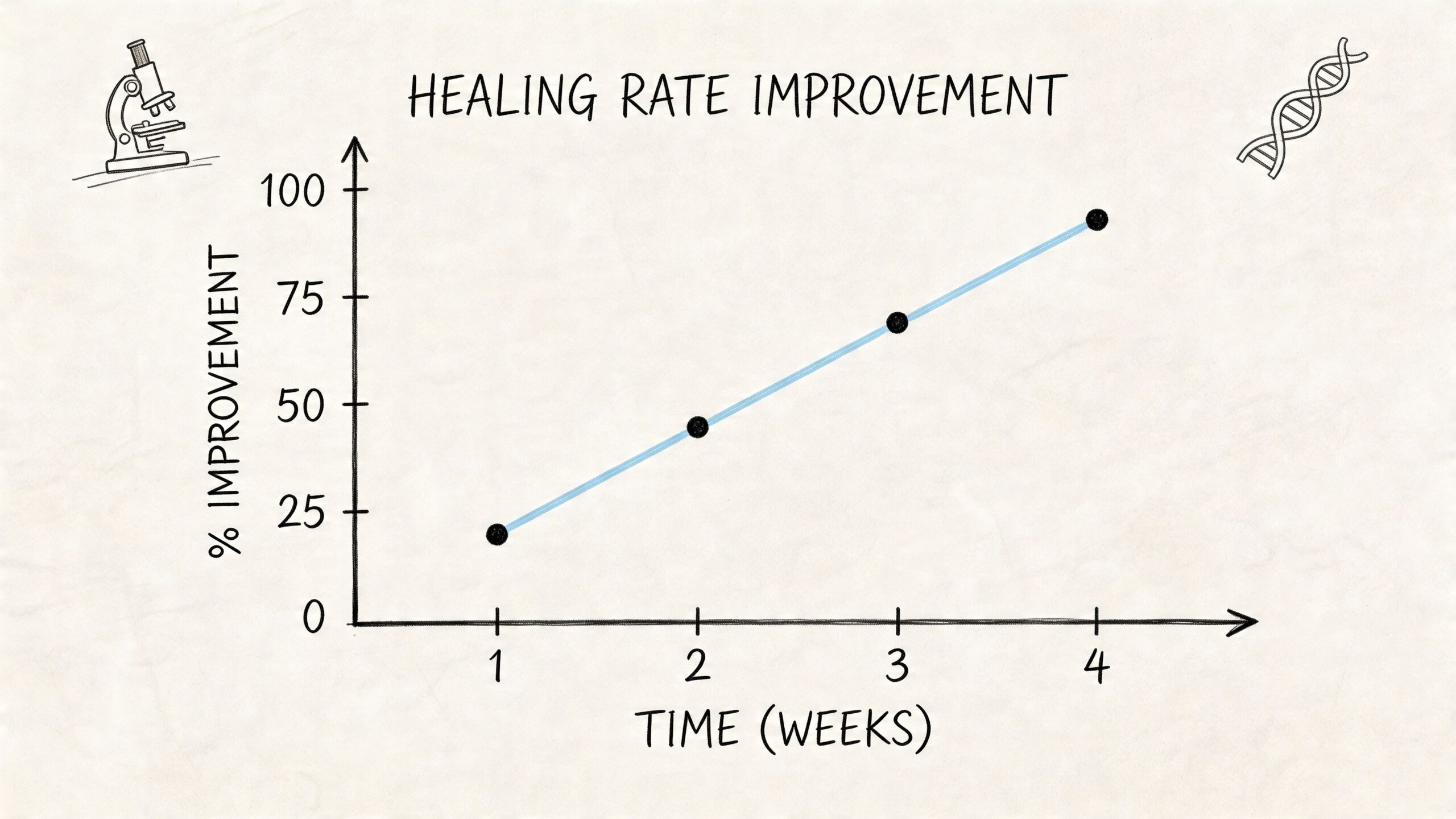
One of the clearest data points comes from a randomized controlled trial summarized in the Healthy Blue medical policy review of MIST Therapy. In that trial, wounds treated with MIST Therapy achieved a 94.9% ± 9.8% wound area reduction over an average of 5.5 ± 2.8 weeks, while the standard of care group achieved 37.3% ± 18.6% reduction over 9.8 ± 5.5 weeks. At 12 weeks, 40.7% of wounds in the ultrasound group reached complete closure versus 14.3% in the sham saline mist group.
Those numbers are meaningful, but they need context. The benefit shows up in selected chronic wounds, not in every wound that happens to be open. Patients still need the rest of the plan handled correctly, including offloading, compression, moisture balance, infection control, and follow-up measurements.
What the evidence means in real practice
For a treating clinician, the most useful endpoint is not whether a device sounds advanced. It is whether the wound starts to change direction. Faster area reduction usually means less exudate to manage, fewer dressing failures, and a lower chance that a superficially stagnant wound will stay in that inflammatory cycle for another month.
Closure also matters for practical reasons. A wound that closes sooner usually means fewer supply needs, less caregiver burden, and less cumulative risk from contamination or repeated trauma. In home-based care, that difference can determine whether a patient stays on track or falls into the common pattern of missed appointments and partial treatment.
A structured evidence-based wound care plan still determines whether mist therapy performs well. The modality should be judged alongside weekly measurements, tissue quality, drainage pattern, pain response, and correction of the cause of the wound.
Not all wound types respond the same way
Published studies and policy reviews support mist therapy most strongly as an adjunct for chronic wounds that have stalled under standard treatment. That includes lower-extremity ulcers, diabetic foot ulcers, and pressure injuries, but the clinical logic differs by wound type.
| Wound context | Why evidence matters clinically |
|---|---|
| Venous leg ulcers | Healing can improve if the wound bed is better prepared, but outcomes still depend heavily on consistent compression and edema control. |
| Diabetic foot ulcers | Earlier progress matters because prolonged wound duration increases the chance of infection, deeper tissue involvement, and recurrent pressure injury. |
| Pressure injuries | Noncontact treatment is useful when pain, frailty, or anatomy makes repeated sharp debridement less practical in the home. |
From a mobile practice standpoint, the evidence is strongest when the treatment can be delivered on schedule. That is one reason this therapy fits home-based wound care. Patients who struggle to travel often miss the very frequency of care that advanced therapies require. If Medicare Part B covers medically necessary wound services and the patient qualifies, bringing treatment into the home can improve adherence in a way that does not show up clearly in trial tables but matters every week in real care.
The limitations of the evidence should stay in view. Some studies had short follow-up periods, small samples, or narrow inclusion criteria. That is enough to justify selective use, not routine use on every chronic wound. The practical standard is response. If the wound is not measurably improving after an appropriate trial, the plan should be reassessed rather than prolonged automatically.
Is Mist Therapy Right for Your Wound
Not every chronic wound needs mist therapy. Some do well with basic moisture management, edema control, offloading, and periodic debridement. Others need a more advanced approach because the wound is painful, stalled, or repeatedly contaminated by surface burden.
The strongest candidates are usually the wounds that have already shown they aren’t progressing with routine care.
Good candidates
Mist therapy for wounds is particularly relevant when the wound has one or more of these features:
- It has stalled despite appropriate care: The dressing regimen may be technically correct, but the wound bed remains fibrotic, inflamed, or minimally progressive.
- Sharp debridement isn’t well tolerated: This is especially important in patients with pain, bleeding risk, frailty, or wound locations that are difficult to access.
- The location is challenging: MIST therapy is particularly indicated for wounds on difficult areas like heels or buttocks, and for patients who are intolerant of sharp debridement, according to the Parkview discussion of chronic wound mist therapy.
- Bioburden appears to be part of the problem: Wounds with recurrent slough, stalled granulation, or suspected biofilm often need more than passive dressings.
The same Parkview source notes that patient selection is critical and that suitability is often determined for wounds larger than 1 cm² with bioburden that has stalled the healing process.
When mist therapy is less likely to succeed on its own
It’s important to set realistic expectations. Mist therapy helps the wound environment. It doesn’t correct every systemic problem driving the wound.
Consider another strategy first, or use mist therapy only as one piece of the plan, when:
- Pressure isn’t controlled: A plantar ulcer won’t heal if the patient continues full pressure without effective offloading.
- Edema remains unmanaged: Venous ulcers need compression. Without it, even a cleaner wound bed often breaks down again.
- Perfusion is critically limited: Severely ischemic wounds may not respond unless blood flow issues are addressed.
- The wound needs a different priority intervention: Some wounds need urgent surgical management, drainage, vascular assessment, or systemic infection treatment before any adjunctive modality becomes useful.
A good candidate isn’t just “someone with a wound.” It’s someone whose wound biology, tolerance, and care setting make non-contact ultrasound a logical next step.
Questions worth asking before starting
Referring clinicians, patients, and caregivers can use a short decision filter:
- Has the wound clearly plateaued with standard care?
- Is pain or anatomy limiting sharp debridement?
- Will the patient also follow the basics, such as offloading, compression, and dressing adherence?
- Can progress be measured week to week?
If the answer is yes to most of those, mist therapy often makes practical sense. If not, the care plan may need a different correction first.
The Patient Experience What to Expect During Treatment
Most patients are relieved by one thing first. Mist therapy is non-contact. They don’t see a blade, they don’t feel scraping, and the treatment usually feels far less invasive than the debridement methods they may already associate with wound care.
In a home or facility setting, that changes the entire tone of the visit. Patients aren’t waiting for transport, sitting in a clinic lobby with a painful leg, or trying to protect a fragile foot ulcer during travel. The clinician comes to the bedside, recliner, or home setup where the wound can be treated with much less disruption.
What a typical visit feels like
A treatment visit usually begins with the same disciplined wound assessment used in any advanced plan. The dressing is removed. The wound is inspected for tissue quality, drainage, odor, undermining, peri-wound change, and signs that the current strategy is or isn’t working. The mist therapy device is then positioned to deliver low-frequency ultrasound through saline mist to the wound surface.
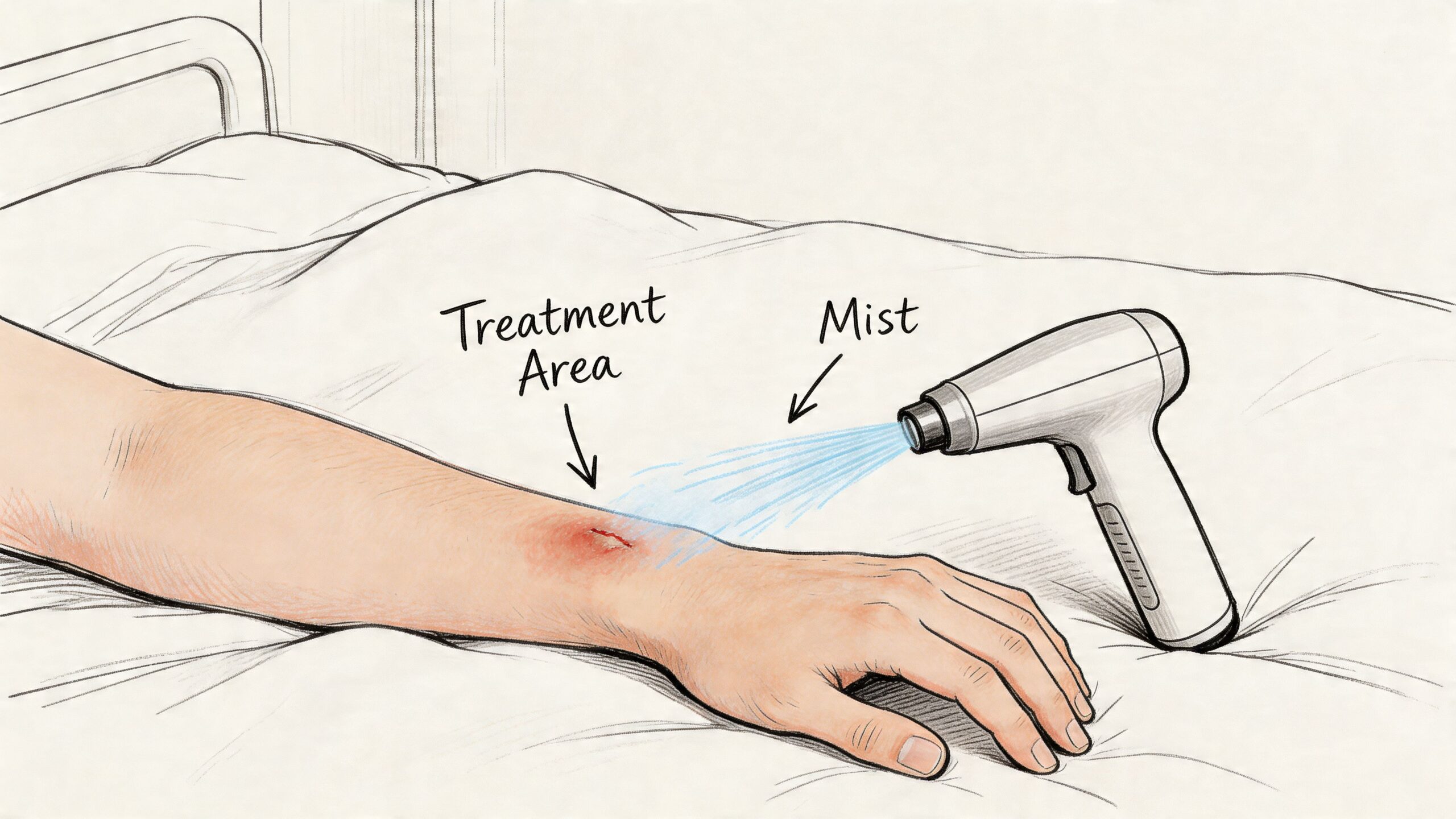
Patients often describe the sensation as gentle airflow or cool moisture rather than pain. That doesn’t mean every wound is sensation-free. A highly inflamed wound can still be tender. But compared with more aggressive mechanical approaches, the experience is usually easier to tolerate.
How often treatment is given
Mist therapy is typically delivered 3 to 5 times per week, a frequency noted in the available clinical and coverage discussion on MIST therapy access and Medicare Part B coverage. That schedule reflects a practical reality in wound care. Chronic wounds often need repeated, consistent intervention rather than occasional rescue treatment.
The key point for patients is consistency. If the treatment is ordered as part of a broader plan, missed visits and inconsistent supportive care can slow the response.
A prospective study reported that when MIST therapy was added, a response was evident within 4 weeks, with a median healing time of 7 weeks, which was 3 weeks faster than historical controls, according to the PubMed report on chronic lower-extremity wounds treated with MIST.
What patients should and shouldn’t expect
Patients should expect:
- A painless or low-discomfort experience in many cases
- Repeated sessions rather than a one-time fix
- Ongoing use with dressings and other wound measures
- Regular reassessment to confirm the wound is improving
Patients shouldn’t expect:
- Immediate closure after a few sessions
- Success if pressure, edema, or blood sugar issues are ignored
- Mist therapy to replace every other part of wound care
The most successful patients usually aren’t the ones getting the fanciest treatment. They’re the ones whose treatment, dressing support, pressure relief, and follow-up all stay aligned.
Accessing Mist Therapy with Windy City Wound Care
One of the least discussed parts of mist therapy for wounds is access. Clinical efficacy matters, but so do the logistics. Can the patient receive treatment consistently? Will the care fit within the home setting or facility workflow? Will insurance support it?
Those questions are where mobile wound care becomes especially relevant for older adults, patients with limited mobility, and post-acute populations.
Why mobile delivery changes adherence
When advanced wound care is brought into the home, assisted living community, or skilled nursing facility, treatment becomes easier to maintain. Patients avoid repeated transportation barriers. Caregivers can see the plan directly. Facility staff and home health teams can coordinate around a wound specialist’s recommendations without waiting for off-site appointments.
That matters because chronic wounds don’t heal on convenience. They heal on consistency.
Coverage and referral realities
A critical gap in online information is cost and coverage. Available information notes that MIST therapy is typically delivered 3 to 5 times per week and is covered under Medicare Part B, making it accessible for eligible seniors in home-based and facility settings, as discussed in the mobile wound care overview for Chicago-area patients.
For referring physicians, discharge planners, podiatrists, and home health agencies, the practical process should be simple:
- Identify the stalled wound: Diabetic ulcers, venous ulcers, pressure injuries, and post-surgical wounds are common referral categories.
- Send the clinical context: Recent measurements, vascular history, infection concerns, offloading or compression status, and prior treatment response all help.
- Coordinate the existing plan: Advanced therapy works better when the specialist, primary team, and caregivers are all reinforcing the same wound goals.
What makes a referral more useful
The strongest referrals usually include a clear reason the wound isn’t progressing. That may be persistent slough, intolerance to debridement, recurrent drainage, painful peri-wound tissue, or repeated setbacks after discharge. A specialist can work from limited information, but better context almost always leads to a more efficient initial plan.
For patients and families, the important takeaway is simple. You don’t need to figure out advanced wound care by trial and error. If a wound has lingered, worsened, or become too difficult to manage through office-based care alone, an in-home evaluation can clarify whether mist therapy belongs in the treatment plan.
Frequently Asked Questions About Mist Therapy
Is mist therapy painful
Usually, it’s well tolerated because it is non-contact. Many patients find it much easier than sharp or mechanical debridement. A very inflamed wound can still be sensitive, but the treatment itself is designed to be gentle.
How soon can you tell if it’s working
Clinicians look for changes in tissue quality, drainage, slough, peri-wound inflammation, and wound measurements over the first few weeks. In the clinical evidence cited earlier, response was evident within a relatively short period in selected chronic wounds. In practice, if a wound isn’t showing meaningful progress, the plan should be reassessed rather than continued indefinitely.
Can mist therapy be combined with compression or offloading
Yes. In fact, it usually should be paired with the fundamentals that match the wound cause. Venous ulcers still need compression. Diabetic foot ulcers still need offloading. Pressure injuries still need pressure redistribution and repositioning.
Is it only for severe wounds
No. The better question is whether the wound is stalled, contaminated, difficult to debride, or poorly tolerated with standard treatment. Some moderate wounds are appropriate. Some very severe wounds need a different first priority, such as vascular or surgical management.
Why does in-home delivery matter so much
Because chronic wound care is repetitive. Home-based treatment reduces travel strain, supports continuity, and lets the specialist assess the environment affecting healing, including footwear, bed surfaces, transfer technique, edema control, and caregiver support.
If you or someone you care for has a chronic wound that isn’t progressing, Windy City Wound Care provides advanced mobile wound care across Chicago and surrounding Illinois counties. Their clinicians treat patients in homes, assisted living communities, and skilled nursing facilities, and they coordinate with physicians, home health agencies, and caregivers to build individualized plans. New patients can call 708-497-9850, and providers can fax referrals to 844-333-1773.
